
Surgical techniques
FETT - flexor tenodesis
PIPJ fusion
Distal metatarsal shortening osteotomy
FDL tenodesis
Indication
Flexible PIPJ
Concept
Flexor tenodesis
- release FDL distally
- attach to dorsal surface of base of P1
Technique


Arthrex surgical technique with biotenodesis screw
Flexor to Extensor Tendon Transfer (FETT) / Modified Girdlestone Taylor
- two incisions
- plantar incision transverse over skin crease
- harvest FDL distally
- splint FDL into two
- dorsal incision
- retrieve tendon slips
- protect neurovascular bundle
- suture to each other other over base of P1
- P1 in 20 degrees of flexion
Technique 2
- single dorsal incision
- in association with PIPJ fusion
- dorsal incision over PIPJ
- open PIPJ
- identify FDL between short flexors and divide
- suture over base of P1
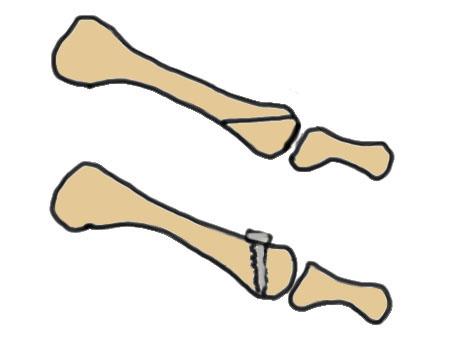
+/- retrieve through drill hole in proximal P1 / biotenodesis screw
Results
Iglesias et al J Am Podiatr Med Assoc 2012
- meta-analysis of FDL transfer
- satisfaction rate 92%
PIPJ fusion




Indication
Fixed PIPJ contracture - hammer toe / claw toe
Technique
Dorsal transverse incision over PIPJ
- longitudinal incisions can cause contractures
- divide extensor tendon
- dorsal capsulotomy
- release the collaterals so that P1 subluxes into operative field
- elevate volar plate off P1
- release FDL / FDB
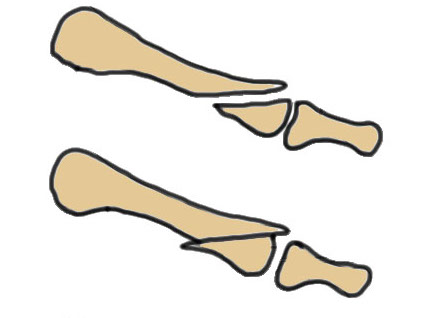
- resect distal P1 / proximal P2
K wire fixation
- retrograde K wire out through P2 and P3 first
- back through P1, rest against subchondral bone
- check K wire position with image intensifier
- bend wire over and tape
+/- intramedullary device
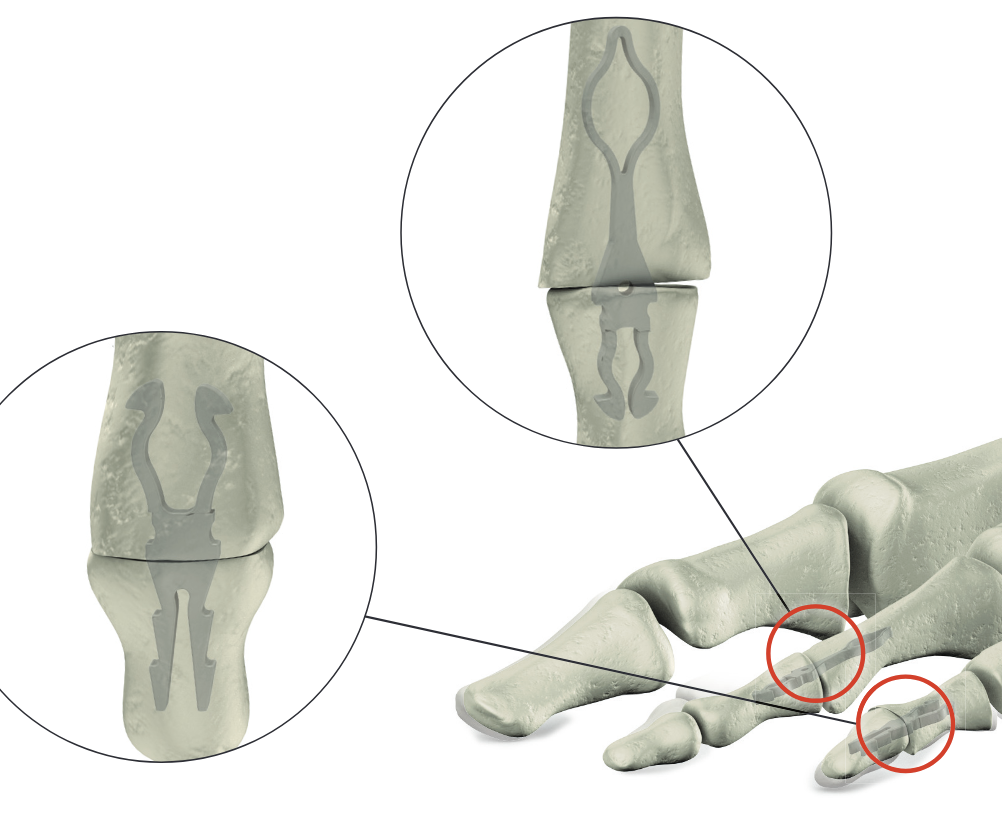
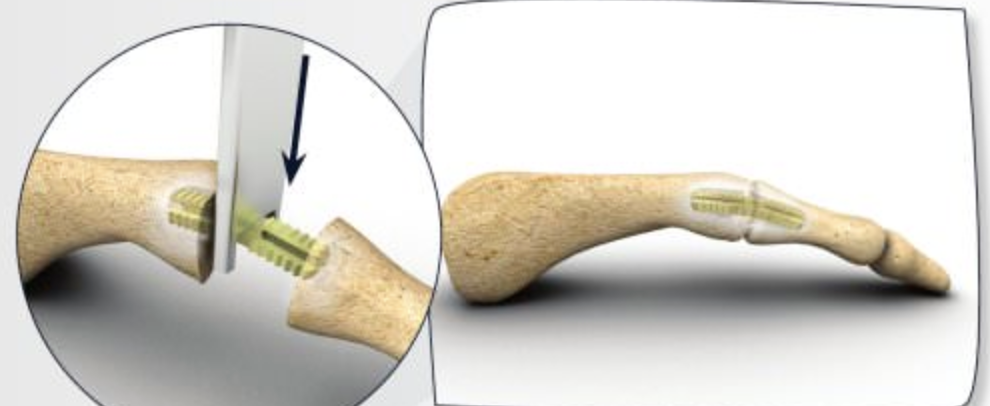
Stryker SmartToe IM device ToeGrip
Results
- PIPJ fusions
- 3000 K wires, 350 SmartToe, 200 ToeGrip
- highest union rate with SmartToe
- highest failure rate with SmartToe
- K wire migration 5%
Ischemia
Let tourniquet down at end of case and check toes
Toe ischemic
- release dressings
- warm patient
- increase BP
- raise head / lower foot
- warm saline dressings
- will usually reperfuse over 5 minutes
- nitroglycerin paste
- adjust k wire
- need to have ischaemia as part of consent
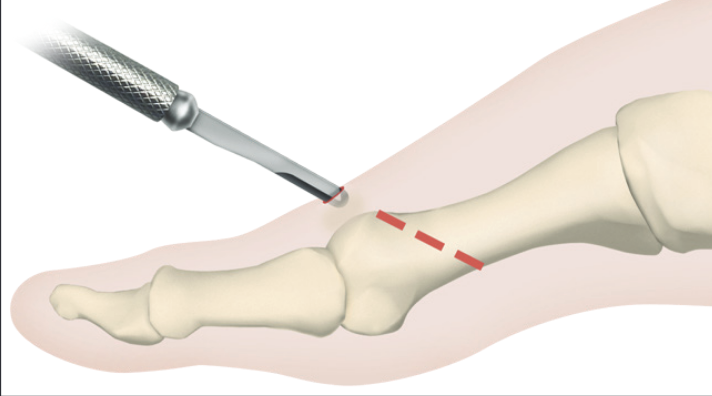
Distal metatarsal shortening osteotomy
Indications
Fixed MTPJ deformity
Options
Weil Osteotomy - intra-articular distal osteotomy
Distal metatarsal metaphyseal osteotomy (DMMO) - extra-articular
Weil Osteotomy


Technique
Dorsal incision over MTPJ
- web space incisions if doing multiple toes
- mobilize EDL tendons
- capsulotomy to expose MTPJ
Osteotomy
- homan retractors each side of metatarsal
- saw enters at edge of articular surface dorsally
- osteotomy parallel to the floor
- when osteotomy complete the MT head slides back
- needs to slide back at least 5mm
- amputate leading edge of proximal fragment
+/- screw fixion
+/- plantar plate fixation
Results
Highlander et al Foot Ankle Spec 2011
- 1100 Weil osteotomy
- 36% floating toe
- recurrence 15%
- transfer metatarsalgia 7%
- delayed union / nonunion 3%
- 278 Weil osteotomy
- 195 fixed with screw - revision rate 25% (primarily MTPJ arthrolysis)
- 83 without screw - revision rate 10%
- no difference in clinical outcome
Fleischer et al J Foot Ankle Surg 2020
- 86 patients with Weil osteotomy
- +/- plantar plate repair
- better outcomes with plantar plate repair
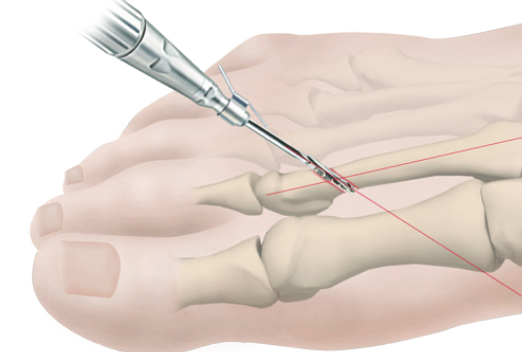
Distal metatarsal metaphyseal osteotomy (DMM)
Technique
Extra-capsular
Shortening
MIS techniques
Results
- meta-analysis of Weil v DMMO
- 4 studies and 200 patients
- no difference in outcomes
Rivero-Santana et al Foot Ankle Surg 2019
- systematic review of Weil v DMMO
- 4 retrospective studies
- DMMO - longer time to bone healing
- Weil - increased stiffness / wound problems
Complications of lesser toe surgery
Ischemia / necrosis / amputation
Infection
Nerve injury
Nonunion
Malunion
MTPJ instability
MTPJ OA